INTRODUCTION
Blunt abdominal trauma (BAT) can be caused by a multitude of etiologies, the most common of which are motor vehicle accidents. 1 BAT can cause damage to the internal organs, resulting in hemorrhage and contusion. Diagnosis often takes place in the emergency department, with a thorough history and physical exam followed by focused assessment with sonography for trauma and CT scan. One outcome of BAT is abdominal hematoma, which usually arises from bleeding between the muscle layers of the abdominal wall. 2 There are two well-known variations of abdominal wall hematoma – rectus sheath hematoma and lateral wall hematoma. Rectus sheath hematoma is much more common than lateral wall hematoma, 3 , 4 but both have the capability of spreading into the abdominal cavity. Hematomas are most often treated conservatively as the expansion stops once significant pressure has built up within the cavity. 2 However, if hemostasis is not achieved within the hematoma, it can continue to expand and irritate local structures, causing pain. Another potential adverse outcome of hematoma is infection of its contents. We present the case of a chronic, infected intra-abdominal hematoma in a janitor. Uniquely, the history of trauma was elicited 9 months after the initial presentation to the ED, and just 1 month before surgery.
CASE
The patient is a 71-year-old male with a history of cholecystectomy who presented to the emergency department in late March 2020 with three days of cough and intermittent, aching right flank pain. He rated the pain as a 6/10. He went to his primary doctor 2 days before for this problem and was found to have blood on urine dipstick. He was sent to the emergency department for x-ray and ultrasound. There, he was afebrile and denied body aches, nausea, vomiting, chest pain, and shortness of breath. He had traveled to his home country of Honduras 5 months earlier. Urinalysis showed moderate blood and no red blood cells. The most likely diagnosis at this time was a renal stone. Appendicitis was the second most likely diagnosis. A CT scan of the abdomen and pelvis with contrast showed ovoid hypodense foci anterolateral to the right hepatic lobe and medial to the inferior right hepatic lobe with the largest measuring 1.7 cm. There was also fusiform enlargement of the right transversus abdominis muscle. These could have been hematomas or infectious processes. There were no renal stones on CT. All labs were within normal limits, and the patient was discharged with a diagnosis of hepatic abscess. Two days later after speaking to radiology and GI, his primary care doctor started him on ciprofloxacin and fluconazole for 28 days. Colonoscopy was arranged to rule out malignancy.
Three months later the patient was still complaining of right upper quadrant pain. He was following with his primary care doctor, who ordered a repeat CT scan that showed no interval changes compared to previous exam. Liver function tests showed mild elevation, with AST of 53 and ALT of 82. The patient was sent to interventional radiology for biopsy, which showed cores of reactive fibroconnective tissue with thick-walled vessels and entrapped skeletal muscle with scattered plasma cell aggregates. These features were compatible with abscess wall. One month later the patient underwent repeat liver function tests along with full hepatitis work up. The transaminitis had resolved and hepatitis workup was negative, but the patient continued to have pain. He was referred to pain management, and ultimately received 3 injections with bupivacaine over the course of the next month for pain relief. The injections only helped him for a couple of days at a time, and the pain persisted.
Repeat CT scan on 11/18/20 showed that the mass had enlarged, along with the anterior right paracardiac lymph node and a lymph node in front of the uppermost liver Figure 1. Because the mass had grown, surgical exploration was required. Thoracic surgery was consulted and a concern for a diaphragmatic tumor developed. It was at this time that a surgical resident asked the patient for more details surrounding his initial presentation. The patient revealed that his initial pain started after a floor polishing machine hit him in the flank. On 12/29/20 the patient was taken for laparoscopic surgery to biopsy the mass. When it was touched, purulent material drained and entered the abdomen. The whole mass was resected. Two weeks post op the patient was seen in clinic, and pathology and culture results were reviewed. The final pathology revealed fibromuscular tissue showing focal inflammatory exudate with scattered foreign body like giant cells, focal chronic inflammation, and surrounding tissue fibrosis. There was no evidence of malignancy. Culture of the exudate grew streptococcus viridans. He did not receive antibiotics because he was afebrile and feeling well. He did not complain of any further pain, and no other scans were ordered.
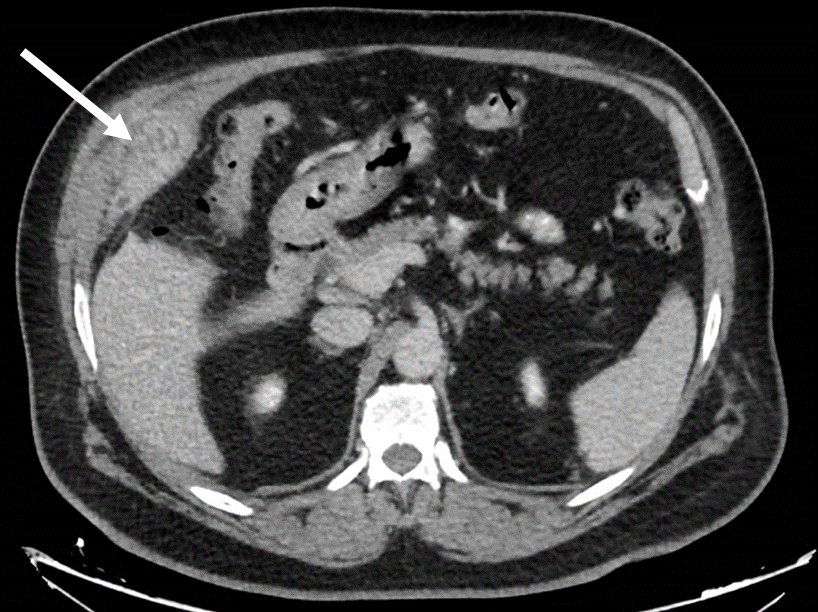
Figure 1. Enlarged mass anterolateral to the right hepatic lobe
DISCUSSION
We report the case of a lateral wall intra-abdominal hematoma that occurred after blunt abdominal trauma to the right flank. The hematoma became infected and grew, causing the patient pain and uncertainty. The hematoma was likely due to venous bleeding near the transversus abdominis muscle because it grew slowly.
3
Part of the blood supply to the transversus abdominal muscle, which was diffusely enlarged on CT scan, are the deep circumflex iliac vessels, which are implicated in lateral wall hematoma.
4
We believe that this patient had a lateral wall hematoma that spread intra-abdominally and became infected, transforming into an abscess that mimicked a diaphragmatic mass. Because of the tumor’s location, diaphragmatic malignancy was considered. Luckily for the patient, diaphragmatic tumors are rare, with only about 150 primary tumors reported in the literature.
5
His initial hematuria was likely due to renal trauma.
We find it especially important to note the importance of taking a good history. Whether the provider is a medical student, resident, or attending, a thorough history with open ended questions should be taken. If the history of trauma was elicited during the initial presentation to the emergency department or in any of the subsequent specialist visits, intra-abdominal hematoma would have likely factored more in the differential. The patient could have had evacuation of the hematoma before it became infected,
6
never having to think about potential cancer.
References
-
O’Rourke MC, Landis R, Burns B. Blunt Abdominal Trauma. In: StatPearls. StatPearls Publishing; 2020. Accessed January 12, 2021. http://www.ncbi.nlm.nih.gov/books/NBK431087/
-
Shikhman A, Tuma F. Abdominal Hematoma. In: StatPearls. StatPearls Publishing; 2020. Accessed January 10, 2021. http://www.ncbi.nlm.nih.gov/books/NBK519551/
-
Dutta S, Sanjay P, Jones ML. Diagnosis and treatment of giant lateral abdominal wall haematoma after blunt trauma: a case report. Cases J. 2009;2:9358. doi:10.1186/1757-1626-2-9358
-
Özden S, Özsoy Y, Yoler L, Erhan Y, Aydede H. Late diagnosis of a lateral abdominal wall hematoma presenting with nonspecific findings: report of a case.
-
Thapar S, Ahuja A, Rastogi A. Rare diaphragmatic tumor mimicking liver mass. World J Gastrointest Surg. 2014;6(2):33-37. doi:10.4240/wjgs.v6.i2.33
-
Trujillo L, Naranjo S, Cardozo A, Alvarez B. Ultrasound-guided percutaneous drainage of a traumatic abdominal wall hematoma in the emergency department. World J Emerg Med. 2012;3(4):308-310. doi:10.5847/wjem.j.issn.1920-8642.2012.04.013