ABSTRACT
Appendicitis is the most common surgical emergency worldwide. It is most often treated with appendectomy. Several studies have evaluated the seasonal variance of appendicitis and found that it most often occurs in the summer months. To our knowledge, no studies have been done for the Bronx, New York population. Ten years of appendectomies at a Bronx community hospital were reviewed to assess the seasonal variance in appendicitis. There were no significant differences between appendicitis by season. Resources should be allocated in a way that assumes that rates of appendicitis do not fluctuate by season.
INTRODUCTION
Appendicitis accounts for 300,000 hospital visits each year, and appendectomy is the most common emergency surgical procedure in the world.
1
Appendicitis is the inflammation of the appendix, often caused by obstruction of the appendiceal lumen by a fecalith or lymphoid hyperplasia.
2
When the intestinal lumen is obstructed, increased intraluminal pressure causes small vessel occlusion and lymphatic stasis, with the wall of the appendix becoming ischemic and necrotic. This can eventually cause perforation of the appendiceal wall,
2
with free perforation causing peritonitis or complications including phlegmon and abscess. Previous investigations into the seasonality of appendicitis have found that appendicitis most often occurs during the summer months of June, July, and August.
3
‘
4
‘
5
‘
6
‘
7
Various theories attempting to explain the increase in appendicitis during the summer months include air pollution,
8
lymphoid hyperplasia secondary to enterovirus outbreak,
5
and low fiber diet.
9
To our knowledge, no study has examined the seasonal variability and epidemiology of acute appendicitis in the underserved, diverse minority population of the Bronx, New York. This population has the highest rates of multiple chronic diseases
10
and poverty
11
in New York City, so we felt it was important to investigate if large population based studies can be applied to this community. As a marker of appendicitis, we looked at the number of appendectomies performed rather than clinical or radiologically diagnosed cases of appendicitis. We hypothesized that there would be seasonal variability in the presentation of patients with acute appendicitis similar to what was seen in prior small studies.
METHODS
Ten years of appendectomies were retrospectively studied in a small, New York City community hospital to determine the seasonal occurrence of appendicitis. Data was obtained via operative log, using surgical appendectomy as a marker of acute appendicitis, and was de-identified prior to inclusion in our database. It was analyzed via excel. Seasons were defined as Autumn being September, October and November, Winter being December, January and February, Spring being March, April and May, and Summer consisting of the months of June, July, and August. These correlate to observed seasons in the Northern Hemisphere.
RESULTS
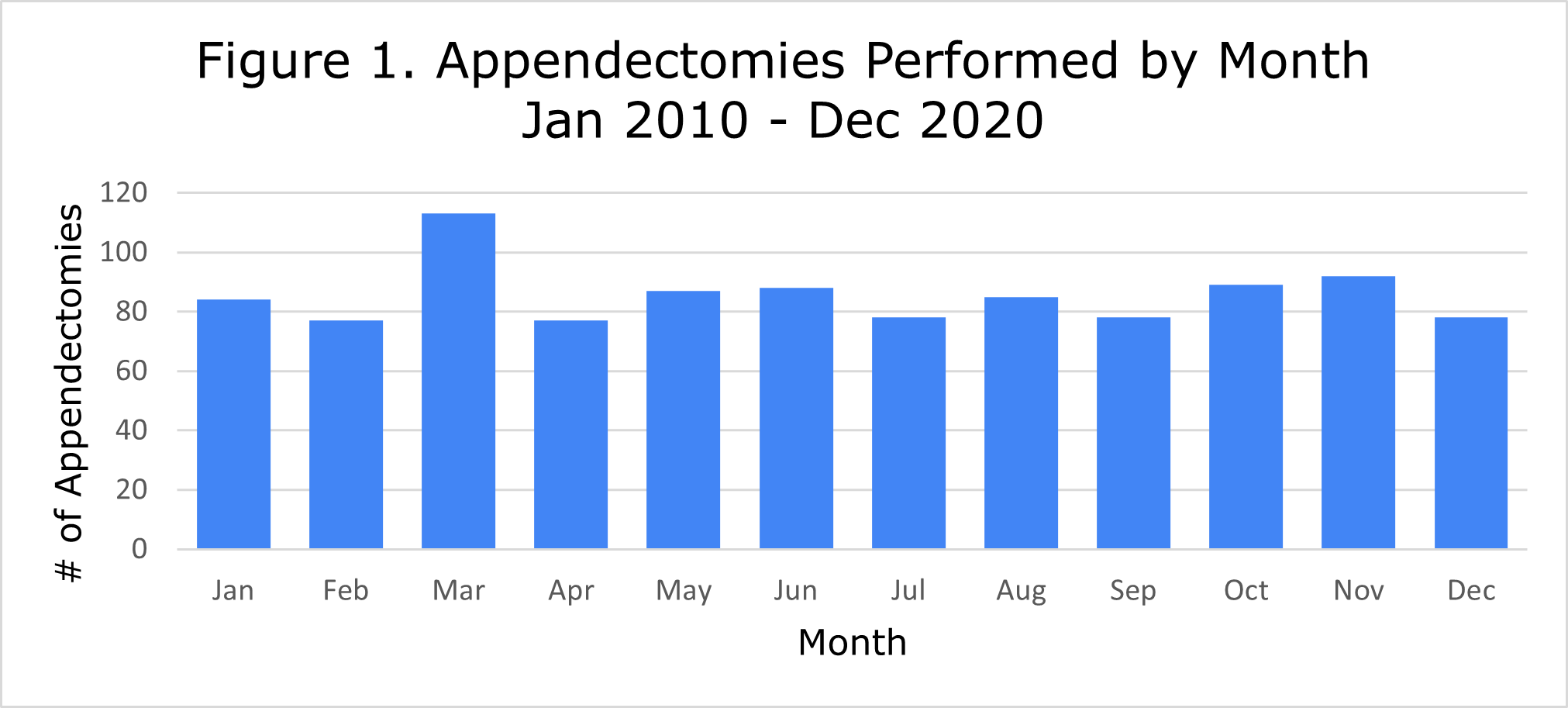
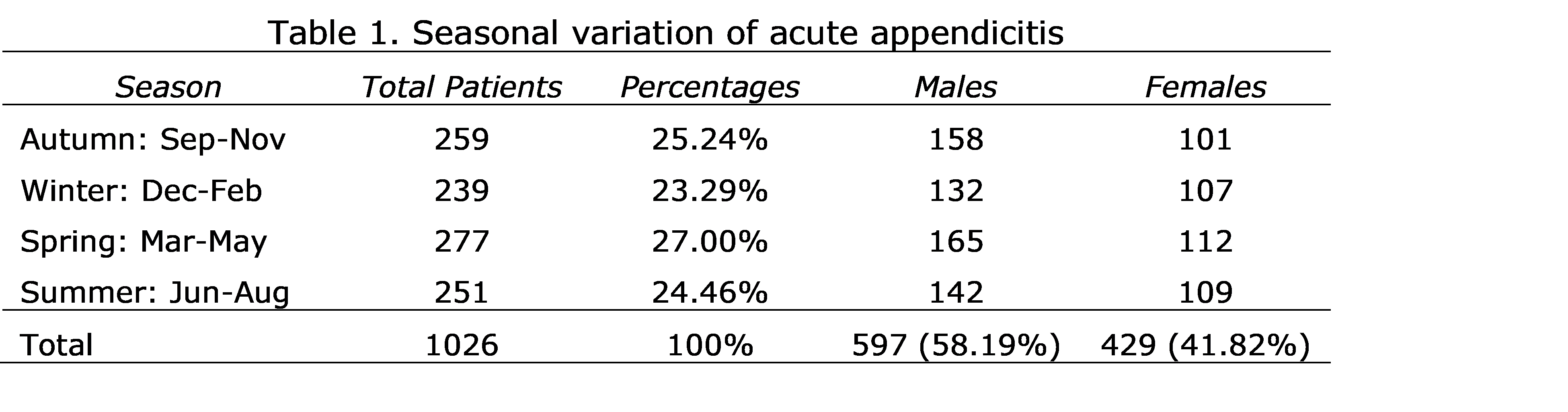
A total of 1026 adult and pediatric patients underwent appendectomy over the ten-year period between January 2010 and December 2020. Of those, 597 (58%) were males, and 429 (42%) were females, and it appears that regardless of season more appendectomies were performed on males. The average male to female ratio was 1.39. The average number of appendectomies performed each year was 102.6. This approximates to between 8 and 9 per month annually. For comparison, 1291 children were diagnosed with acute appendicitis at three large, New York City academic medical centers in the five and a half year period between January 1, 2014, and June 1, 2019. 12 This averages out to about 78 appendectomies per year at each institution. The month with the highest number of appendectomies was March, with 113 appendectomies. The fewest cases were in February and April with 77 appendectomies during each month. Figure 1 is a graphical depiction of the number of appendectomies performed every month. There was no seasonal variation in the number of appendectomies in our patient population. 25% of cases occurred in each quarter (Table 1).
DISCUSSION
Previous studies have shown variability in the incidence of acute appendicitis, with the highest incidence in the summer.
13
In Pakistan, this has been attributed to intestinal parasitic and bacterial infections that peak in the summer causing lymphoid hyperplasia, and thus an association between higher temperature and higher risk of developing acute appendicitis emerged.
6
Additionally, an Indian study showed that the most cases occurred in August and the least in January.
14
This study dealt with acute appendicitis in children, however. Similarly, prior studies have shown that males were diagnosed with acute appendicitis more often than females.
3
‘
5
‘
6
‘
7
This is consistent with the slightly higher lifetime risk of appendicitis in males compared to females.
2
In our study, more males were operated on than females.
The ratio of males to females in our study falls in between those in other studies (range 1.08-4),7,14 but is most similar to the study from Pakistan,
6
with a ratio of 1.42. Our study differs from other studies in that we evaluated appendectomies, rather than cases of appendicitis. We found no significant difference between the number of appendectomies performed during each season. Our results are similar to a study done in New Jersey, which found a non-significant increase in the spring-summer season.
15
They also looked at appendectomies rather than appendicitis. Their study found no statistically significant variation in appendectomies by season, which is potentially due to similar regional
16
and climate
17
exposures in New Jersey as in the Bronx, New York. Instead, they suggest that many variables can influence the incidence of acute appendicitis during the year.
18
One possible explanation for our results is that the Bronx is heavily polluted, especially in the air. Pollution likely does not vary as much from season to season when compared to other areas. Another explanation could be that the population surrounding the hospital lives in unsanitary conditions that predispose to gastrointestinal infections year-round. Also, there is seasonal variability in viral pathogens present that may contribute to finding of trending toward increased numbers during the Autumn and Spring. Students return to school in Autumn, while many suffer from allergies in the Spring. Patients in the Bronx are the poorest in the New York City and thus are more predisposed to negative health outcomes due to their numerous comorbidities.
LIMITATIONS
Our study has its limitations. First, compared to some of the larger studies, our sample size of 1026 is small. 13 This limits the conclusions that can be drawn from the study. Second, the majority of studies in the literature assess cases of acute appendicitis rather than number of appendectomies. However, we feel that number of appendectomies is a good proxy for appendicitis because the vast majority of cases of acute appendicitis are treated surgically with appendectomy as the standard of care in our region. One could argue that cases were missed due to treatment via drainage. However, these patients would have returned for interval appendectomy, and there were only 2 interval appendectomies in 2020 in our hospital. Therefore, we are confident in our use of appendectomy as a proxy for appendicitis.
CONCLUSION
Appendicitis is the most common surgical emergency worldwide. Prior studies have shown an increase in the incidence of appendicitis in the summer months. However no studies have been done in our Bronx population that has numerous comorbidities and lives in poverty. From our research, the rate of appendicitis does not show seasonal variability throughout the year. Further research would be needed to assess the etiology of appendicitis by season, as there may be different viral pathogens at play during different seasons. Additionally, the underlying pathology should be investigated as well, as pathology reports occasionally show mucinous adenomas and chronic appendicitis as opposed to acute inflammation.
REFERENCES
-
Nshuti R, Kruger D, Luvhengo TE. Clinical presentation of acute appendicitis in adults at the Chris Hani Baragwanath academic hospital. Int J Emerg Med. 2014;7:12. doi:10.1186/1865-1380-7-12
-
Jones MW, Lopez RA, Deppen JG. Appendicitis. In: StatPearls. StatPearls Publishing; 2020. Accessed January 27, 2021. http://www.ncbi.nlm.nih.gov/books/NBK493193/
-
Stein GY, Rath-Wolfson L, Zeidman A, et al. Sex differences in the epidemiology, seasonal variation, and trends in the management of patients with acute appendicitis. Langenbecks Arch Surg. 2012;397:1087-1092. doi:10.1007/s00423-012-0958-0
-
Ilves I, Fagerström A, Herzig K-H, Juvonen P, Miettinen P, Paajanen H. Seasonal variations of acute appendicitis and nonspecific abdominal pain in Finland. World J Gastroenterol WJG. 2014;20:4037-4042. doi:10.3748/wjg.v20.i14.4037
-
Hsu Y-J, Fu Y-W, Chin T. Seasonal variations in the occurrence of acute appendicitis and their relationship with the presence of fecaliths in children. BMC Pediatr. 2019;19:443. doi:10.1186/s12887-019-1824-9
-
Ahmed W, Akhtar MS, Khan S. Seasonal variation of acute appendicitis. Pak J Med Sci. 2018;34:564-567. doi:10.12669/pjms.343.14793
-
York TJ. Seasonal and climatic variation in the incidence of adult acute appendicitis: a seven year longitudinal analysis. BMC Emerg Med. 2020;20:24. doi:10.1186/s12873-020-00321-2
-
Kaplan GG, Dixon E, Panaccione R, et al. Effect of ambient air pollution on the incidence of appendicitis. CMAJ Can Med Assoc J. 2009;181:591-597. doi:10.1503/cmaj.082068
-
Adamidis D, Roma-Giannikou E, Karamolegou K, Tselalidou E, Constantopoulos A. Fiber intake and childhood appendicitis. Int J Food Sci Nutr. 2000;51:153-157. doi:10.1080/09637480050029647
-
Newman D, Levine E, Kishore SP. Prevalence of multiple chronic conditions in New York State, 2011–2016. PLoS ONE. 2019;14. doi:10.1371/journal.pone.0211965
-
Wadhera RK, Wadhera P, Gaba P, et al. Variation in COVID-19 Hospitalizations and Deaths Across New York City Boroughs. JAMA. 2020;323:2192-2195. doi:10.1001/jama.2020.7197
-
Fisher JC, Tomita SS, Ginsburg HB, Gordon A, Walker D, Kuenzler KA. Increase in Pediatric Perforated Appendicitis in the New York City Metropolitan Region at the Epicenter of the COVID-19 Outbreak. Ann Surg. 2021;273:410-415. doi:10.1097/SLA.0000000000004426
-
Fares A. Summer Appendicitis. Ann Med Health Sci Res. 2014;4:18-21. doi:10.4103/2141-9248.126603
-
Jangra B, Jangra MS, Rattan KN, Kadian YS. Seasonal and day of week variations in acute appendicitis in north Indian children. J Indian Assoc Pediatr Surg. 2013;18:42-43. doi:10.4103/0971-9261.107021
-
Wolkomir A, Kornak P, Elsakr M, McGovern P. Seasonal variation of acute appendicitis: a 56-year study. South Med J. 1987;80:958-960. doi:10.1097/00007611-198708000-00006
-
Anderson JE, Bickler SW, Chang DC, Talamini MA. Examining a Common Disease with Unknown Etiology: Trends in Epidemiology and Surgical Management of Appendicitis in California, 1995–2009. World J Surg. 2012;36:2787-2794. doi:10.1007/s00268-012-1749-z
-
Zhang Y, Lyu F, Kang Q, et al. Association of meteorological factors with pediatric acute appendicitis in China. Medicine (Baltimore). 2018;97:e12913. doi:10.1097/MD.0000000000012913
-
Taneja N. INCIDENCE OF ACUTE APPENDICITIS – OBSERVED SEASONAL DIFFERENCES. Med J Armed Forces India. 1996;52(4):274-275. doi:10.1016/S0377-123730893-6