Abstract
Cryptococcal Meningitis (CM) associated immune reconstitution inflammatory syndrome (IRIS) has been described as aseptic meningitis with elevated intracranial pressure (ICP). It remains a diagnosis of exclusion. This is a case report of a 52-year-old male patient with newly diagnosed human immunodeficiency virus-1 (HIV) and CM who had initial improvement to induction and consolidation therapy of CM and antiretroviral therapy (ART). However; he deteriorated again and work up revealed multifocal lacunar strokes. Recurrence of CM was ruled out and IRIS diagnosis was presumed. The institution of steroid therapy had a dramatic effect on clinical status. According to our best knowledge, this is the second documented case of CM-IRIS induced stroke. Thus, this case serves to support the prior suggestion in medical literature of IRIS induced stroke.
Case Report
A 52-year-old male patient presented to the emergency department (ED) for altered mental status and lethargy on a background of intravenous drug abuse and recent weight loss. On physical exam, he was oriented only to self, with intact muscle power and brisk deep tendon reflexes. Brain magnetic resonance imaging (MRI) was unremarkable. Past medical history was significant only for smoking without a history of diabetes, hypertension or dyslipidemia. HIV PCR was reactive. Blood culture was unremarkable. HIV viral load was 69,000 copies/ml and CD4 count was undetectable. Cryptococcus neoformans was cultured in the blood. CSF cryptococcal antigen titer was elevated at 1:2560 (reference is less than 1:5) with the findings shown in Table 1. Opening pressure was elevated at 46 cmH2O. The patient completed two weeks of liposomal amphotericin B in combination with flucytosine. His neurological function returned to his baseline. A repeat cerebrospinal fluid analysis (CSF) at the end of the 2 weeks treatment with amphotericin and flucytosine showed a negative CSF culture with white blood cells (WBC) of 50 cells/ml and protein of 154 mg/dl, with opening pressure of 26 cmH2O (see Table 1). Antiretroviral therapy (ART) was started after the 2 weeks treatment and CD4 count at time of ART initiation was zero. He was transitioned to fluconazole 800 mg daily and discharged home one week later. Prophylaxis for both Pneumocystis carinii and Mycoplasma avium was started.
Nine weeks later and while on fluconazole 400 mg daily, he presented again with altered mental status as he was progressively confused and not able to recognize family members. Physical exam showed a thin built, obtunded, nonverbal patient who does not follow commands but withdraws to pain. He was afebrile and vital signs were stable. Labs were largely unremarkable except for bandemia at 62% (reference 0-8%). White blood cell count (WBC) was within normal limits at 7,600 cells/ml and electrolytes were within normal range. At this point 10 weeks after initiation of ART, a repeat CD4 count was 34 cell/ml with undetectable viral load. Brain MRI showed new areas of restricted diffusion in both cerebral and cerebellar hemispheres and corpus callosum with corresponding fluid attenuated inversion recovery (FLAIR) hyperintensities, suggestive of new multifocal areas of infarction with progression of diffuse leptomeningeal enhancement (Figure 1,2). The patient had a lumbar puncture (LP) in a left lateral decubitus position that showed colorless CSF with elevated opening pressure of 30 cmH2O, closing pressure of 8 cmH2O, 52 WBC, elevated protein at 159 mg/dl, and low glucose at 29 mg/dl. Peripheral blood glucose level was at 105 mg/dl. CSF cryptococcal antigen titer was elevated at 1:1280 (reference is less than 1:5). Around 25 ml of clear colorless CSF was removed. CSF cultures including fungal, bacterial, anaerobic and acid fast bacilli were negative. CRP was elevated at 6.2 mg/l (see Table 1).
Table 1
CSF testing for JC virus, herpes simplex virus, cytomegalovirus (CMV) and Varicella zoster virus (VZV) was negative. Workup including transthoracic and transesophageal echocardiography with agitated saline study ruled out cardioembolic origin and cardiac shunt. Magnetic resonance angiography (MRA) revealed significant stenosis of left M2 and left A1/A2 junction (Figure 3). This was demonstrated also by computed tomography angiography (CTA) of the head (Figure 3). He had 3 large volume (38, 45 and 40 ml) LPs in total 4-6 days apart with persistent elevated opening pressure above 35 cmH2O that necessitated lumbar drain (LD) placement. Recurrence of CM was ruled out by negative CSF fungal culture and gram stain. Despite CSF diversion, no significant clinical improvement was appreciated and LD was removed. Also, CSF acid fast bacilli culture and meningitis/encephalitis panels were negative. At this point two weeks into his second admission, IRIS was suspected and he was started on dexamethasone. Within four days, a clinically measurable improvement was appreciated in terms of intermittent ability to follow commands and verbalize with dysarthria. Over the course of one week, his speech and muscle strength significantly improved to 5/5 all extremities except the left upper extremity 2/5. Dexamethasone was continued for a total of six weeks of slow tapering. ART was continued. Dysarthria improved mildly but continued to persist on two months’ follow up. No follow up MRI was obtained due to patient’s refusal.
Figure 1
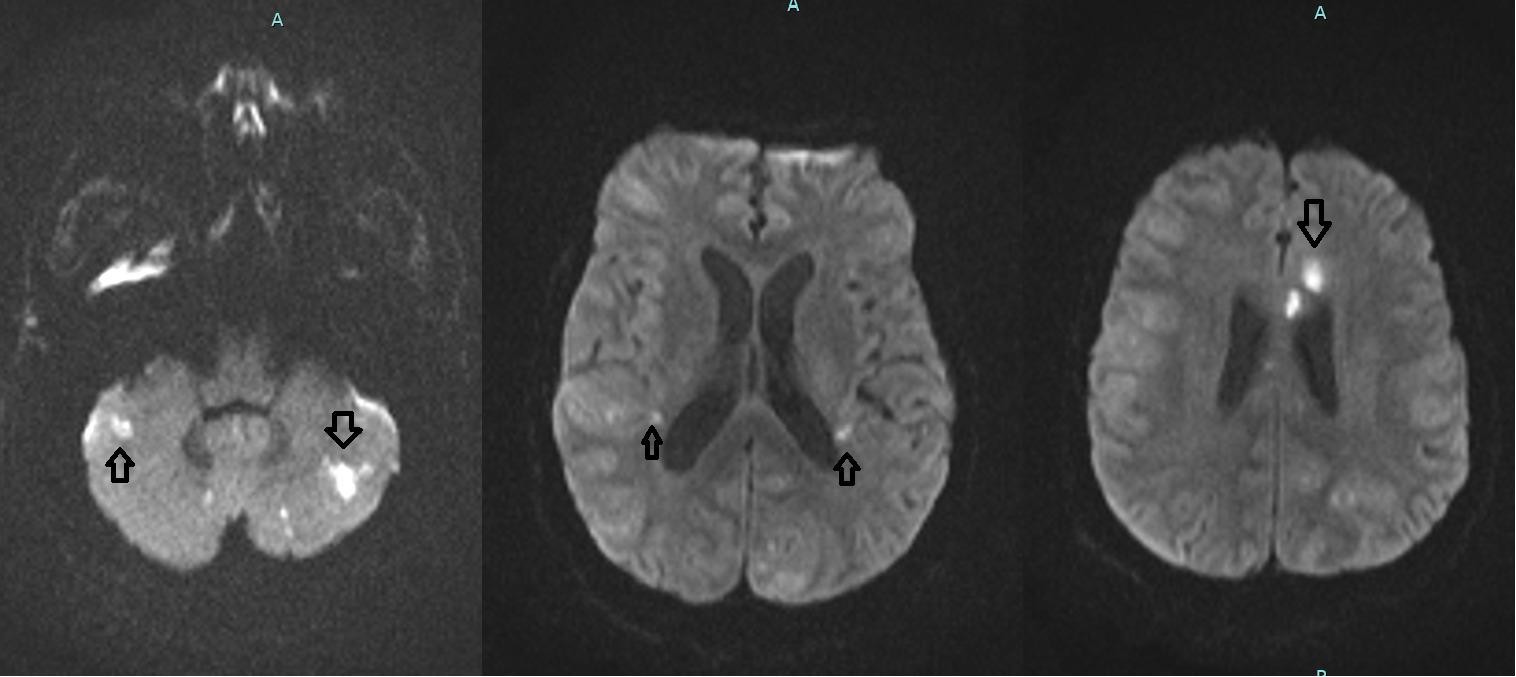
Legend: Diffusion weighted magnetic resonance imaging ( DW-MRI ) brain that shows new diffusion restricted areas suggestive of new lacunar strokes (arrows)
Figure 2
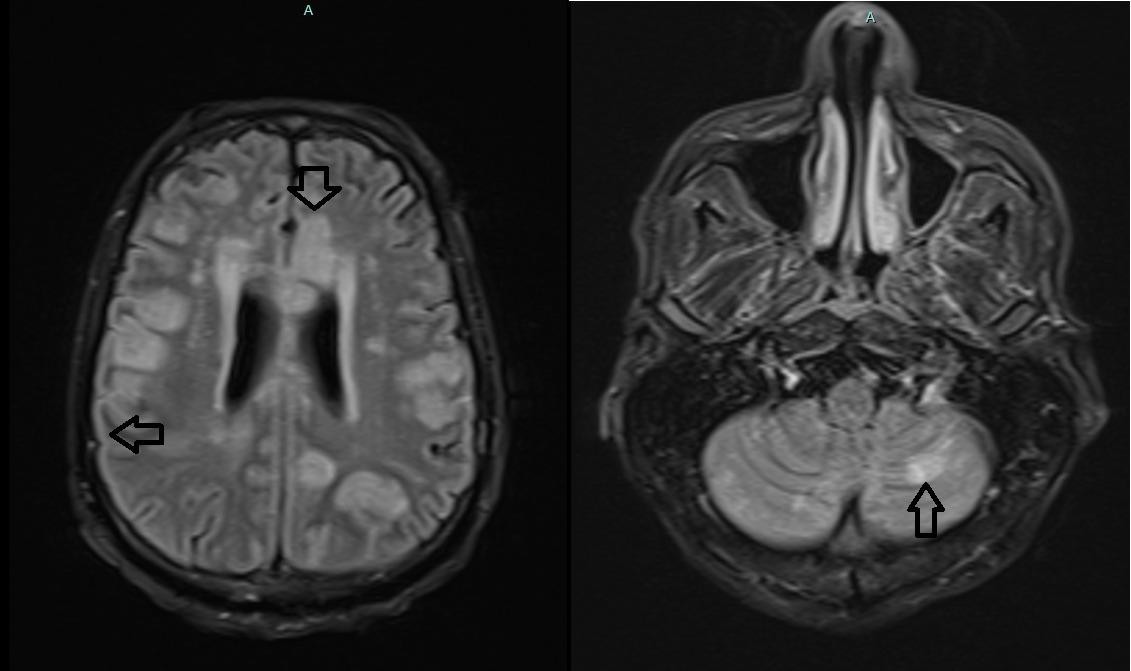
Legend: FLAIR MRI showing new areas of hyperintensity as well as hyperintensity along sulci and gyri (arrows).
Figure 3

Legend: CTA on the left showing areas of stenosis at proximal left MCA and left A1/A2 junction. MRA on the right showing areas of stenosis along the left A1/A2 junction and distal branches of the right MCA.
Discussion
Pathogenesis of IRIS is based on imbalance between regulatory CD4 T cells (Th17) and pro-inflammatory CD4 T cells. 1 IRIS is an important early complication of CM. IRIS is induced by reactivation of immune responses specific to cryptococcus. In this setting, it has two types, paradoxical and unmasking. In the paradoxical, there is worsening of clinical picture after initiation of ART despite initial improvement of CM and characterized by paucity of microorganisms in the CSF. In the second type, CM presents after initiation of ART in those with no prior diagnosis. 1
In this case, factors that support IRIS diagnosis include sterile CSF, increased CSF opening pressure and elevated CSF WBC count. The observation of dramatic clinical improvement in response to steroids also supports the diagnosis of IRIS. Furthermore, IRIS was likely of paradoxical type as indicated by initial improvement of signs and symptoms of CM. Recurrence of CM was effectively ruled out by negative CSF culture and stain as well as lack of response to re-institution of amphotericin and flucytosine. Findings on MRA and CTA along with new areas of restricted diffusion on MRI indicate areas of infarction secondary to vascular stenosis. This allows us to hypothesize that IRIS was a possible trigger of the vascular insults. The main mechanism is believed to be infectious vasculitis that leads to endarteritis obliterans.
2
To the best of our knowledge, this is the second case report in English literature of IRIS-induced stroke.
3
In contrast to our case, ART was delayed and started at week 4.
Even without IRIS, the risk of stroke is already elevated in those with HIV especially in the first 6 months after initiation of ART for multiple factors including HIV associated vasculopathy, infectious vasculitis, and coagulopathy as was demonstrated by a case control study involving 222 patients.
4
HIV is known to be associated with endothelial dysfunction and can lead to vasculopathy in the form of accelerated atherosclerosis and small vessel disease.
4
Also risk of stroke is elevated among those with cryptococcal meningitis as was shown by an Indian retrospective study of 66 patients. It showed that 13% of them had strokes, all of which were lacunar strokes and most commonly in basal ganglia. Male predominance and multiple lacunes were observed. Prognostic significance to vascular injury was also evident.
5
This was confirmed by another retrospective study in the US. Also in this study, certain predictors of stroke were suggested including hyponatremia, anemia and malignancy.
6
Risk factors of CM-IRIS include initiation of ART within 30-60 days after diagnosis of CM, fungemia and low CD4 count 7 . Paucity of CNS inflammation as indicated by CSF WBC count less than 25 cell/ml and protein less than 50 mg/dl is associated with a sevenfold higher risk of CM-IRIS. 8 Also, CSF culture positivity before starting ART is associated with threefold higher risk of CM-IRIS. 9 Elevated CRP more than 32 mg/dl is also an indicator of higher risk of CM-IRIS. 10 Recommendations to lower the risk of CM-IRIS include achieving CSF sterility before transition from fungicidal to fungistatic therapy either by prolonging initial induction therapy or adding flucytosine, or fluconazole at doses higher than 800 mg daily. Although initial data from the AIDS Clinical Trials Group A5164 strategy trial did not find benefit of delaying ART initiation, a more recent larger randomized trial involving 177 subjects showed significant mortality benefit of delaying ART 5 weeks as compared to 1-2 weeks in CM 10 . A meta-analysis of 4 randomized control trials confirmed the mortality benefit of delayed ART in CM, though it was uncertain if it is related to lower IRIS rates. 11
Mortality rate of CM-IRIS is higher than other types of IRIS, 20.8% compared to 3.2% in tuberculosis associated IRIS and 4.5% for any type of IRIS. 12 Management of IRIS includes continuation of ART and alleviation of elevated ICP. For severe IRIS with CNS complications including symptomatic elevated ICP and neurological deficits, Infectious Disease Society of America guidelines (IDSA) recommend steroids tapered over 2-6 weeks. 13 In refractory cases, some case reports suggested effective use of thalidomide or adalimumab. 14
References
-
Haddow LJ, Colebunders R, Meintjes G, Lawn SD, Elliot JH, Manabe YC, et al. Cryptococcal immune reconstitution inflammatory syndrome in HIV-1-infected individuals: proposed clinical case definitions. Lancet Infect Dis 2010; 10:791–802
-
Martin-Blondel G, Delobel P, Blancher A, Massip P, Marchou B, Liblau RS, et al. Pathogenesis of the immune reconstitution inflammatory syndrome affecting the central nervous system in patients infected with HIV. Brain 2011; 134: 928–46
-
Ellis JP, Kalata N, Joekes EC, Kampondeni S, Benjamin LA, Harrison TS, et al. Ischemic stroke as a complication of cryptococcal meningitis and immune reconstitution inflammatory syndrome: a case report. BMC Infect Dis 2018; 18: 520
-
Benjamin LA, Corbett EL, Connor MD, Mzinganjira H, Kampondeni S, Choko A, et al. HIV, antiretroviral treatment, hypertension, and stroke in Malawian adults: a case-control study. Neurology 2016; 86: 324–33
-
Mishra AK, Arvind VH, Muliyil D, Kuriakose CK, George AA, Karuppusami R, et al. Cerebrovascular injury in cryptococcal meningitis. Int J Stroke 2018; 13: 57-65
-
Vela-Duarte D, Nyberg E, Sillau S, Castellanos P, Chastain DB, Franco-Paredes C, et al. Lacunar strokes in cryptococcal meningitis: clinical and radiographic features in a U.S. cohort. Neurology 2019; 92: P4.3-015
-
Sungkanuparph S, Jongwutiwes U, Kiertiburanakul S. Timing of cryptococcal immune reconstitution inflammatory syndrome after antiretroviral therapy in patients with AIDS and cryptococcal meningitis. J Acquir Immune Def Syndr 2007; 45: 595–596
-
Chang CC. Patients with cryptococcal meningitis who attain CSF sterility pre-ART commencement experience improved outcomes in the first 6 months. Paper presented at: 8th International Conference on Cryptococcus and Cryptococcosis; May 5, 2011; Charleston, SC
-
Boulware DR, Meya DB, Bergemann TL, Wiesner DL, Rhein J, Musubire A, et al. Clinical features and serum biomarkers in HIV immune reconstitution inflammatory syndrome after cryptococcal meningitis: a prospective cohort study. PLoS Med 2010; 7: e1000384
-
Boulware DR, Meya DB, Muzoora C, Rolfes MA, Huppler Hullsiek K, Musubire A, et al. Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis. N Engl J Med 2014; 370: 2487-98
-
Eshun-Wilson I, Okwen MP, Richardson M, Bicanic T. Early versus delayed antiretroviral treatment in HIV-positive people with cryptococcal meningitis. Cochrane Database Syst Rev 2018; 7: CD009012
-
Muller M, Wandel S, Colebunders R, Attia S, Furrer H, Egger M, et al. Immune reconstitution inflammatory syndrome in patients starting antiretroviral therapy for HIV infection: a systematic review and meta-analysis. Lancet Infect Dis 2010; 10: 251–61
-
Perfect JR, Dismukes WE, Dromer F, Goldman DL, Graybill JR, Hamill RJ, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america. Clin Infect Dis 2010; 50: 291–322
-
Brunel AS, Reynes J, Tuaillon E, Rubbo PA, Lortholary O, Montes B, et al. Thalidomide for steroid-dependent immune reconstitution inflammatory syndromes during AIDS. AIDS 2012; 26: 2110–2