Abstract
Skin graft and flaps have become common practice in the plastic surgery specialty and have been demonstrated as safe and effective surgical procedures. The most common indications for a skin graft or flap is a third degree burn, chronic ulcer and trauma. Skin graft failure may occur for a variety of reasons, with incidence reported between 2 and 30%. There are currently no studies on the effect of osteopathic manipulative treatment (OMT) on skin graft failure. A retrospective chart review of electronic medical records for thirty-three patients who underwent a skin graft or skin flap procedure from January 1, 2010 to December 31, 2015 at a community based hospital in the Bronx, NY was conducted. Variables which increase the likelihood of graft and flap failure such as immunodeficiency, polytrauma, substance abuse as well as flap and graft complications were collected and treatment patients were matched to controls for such variables. Twelve patients received osteopathic manipulative treatments and twenty-one patients did not. None of the skin grafts or flaps failed in the patients who received OMT as compared to four graft or flap failures in those who did not receive OMT. We feel the lack of statistical significance is due to the low study population. The data, however, is promising and suggests a potential role for OMT in flap and graft patients. This study indicates the need for further research into the effectiveness of OMT in the prevention of flap and graft failure.
Introduction
The surgical technique of skin grafting was initially documented in India 2500 to 3000 years ago to improve the cosmetic appearance of those who had sustained an amputation, most often after committing a crime such as adultery or theft. 1 Skin grafts and flaps have become common practice within the plastic surgery specialty and flaps have been consistently demonstrated as safe and effective surgical procedures. The most common indication necessitating a skin graft or flap is a third degree burn requiring surgical intervention. 1 Chronic ulcers, trauma and elective skin grafts and flaps are other common indications. 1 Varied data on the rates of total skin graft or flap failure is present in the literature with ranges between two and thirty percent. 2 , 3 The most common complication, which leads to skin graft failure, is development of a hematoma which prevents perfusion to the donor graft. 4 , 5 The most common complication causing skin flap failure is necrosis of the most distal portion of the flap, most often due to mechanical forces. 6 , 7 There are multiple other causes of graft and flap failure which include seroma, infection, rejection (xenograft), and instability (mechanical shearing force). 4 , 5 , 6 While most failed skin grafts/flaps do not necessitate exploration and are able to heal via secondary intention, there is an increased duration of healing as well as adverse cosmetic implications. 2 , 3 Additionally these complications increase duration of hospital stay, risk of infection and cost of care. 2
Neuromusculoskeletal medicine (NMM) is a medical specialty pursued by osteopathic physicians with extensive knowledge of anatomy, physiology and pathology. 8 Osteopathic Manipulative Treatment (OMT) is the manual treatment of a patient, utilizing non-invasive techniques most commonly performed by NMM specialists and other osteopathic physicians. OMT is the application of manual external forces with intent to identify and treat somatic dysfunction. 8 A somatic dysfunction is defined as an “impaired or altered function of related components of the somatic (body framework) system: skeletal, arthrodial, and myofascial structures, and related vascular, lymphatic, and neural elements.” 1 The application of osteopathic treatment is believed to improve systemic responses to injury via mechanisms such as metabolism, circulation, intestinal motility, cardiac function and pulmonary response. Local responses include improvement in venous and lymphatic drainage and decreased pain response. 7
The current literature demonstrates a positive correlation in patients who have received physiotherapy and scar massage to skin graft success. 5 Furthermore, the use of osteopathic manipulative treatment has been demonstrated to improve chronic wound healing. 9 As previous success with other modes of manual techniques have demonstrated improved outcomes, further exploration into utility of this form of intervention is necessary. To date there has been no study with intention to evaluate the efficacy of OMT in the setting of patients who have received a skin graft or flap. This retrospective study will serve as a platform to demonstrate the need for more extensive research with regards to graft and flap success in those who received OMT. The intention of this study is to assist in the continued improvement of care to patients and further establish OMT as an adjunct medical intervention with utility in the postoperative patient.
Methods
A retrospective chart review of electronic medical records for thirty-three patients who underwent a graft or flap procedure from January 1, 2010 to December 31, 2015 at a level two trauma center in a Bronx, New York hospital was performed. A list of all postoperative patients within the plastic surgery department was compiled. All patient charts with graft or flap procedures completed within the above timeframe were reviewed in their entirety. Data regarding hospital stay, comorbid medical conditions, complications of graft as well as type of graft or flap and whether it was successful was compiled for patients who had received OMT as well as for those who did not receive OMT. Rates of graft and flap failure were compared in those who received OMT to those who did not. Every attempt was made to match patients who received treatment to those who did not to control for variables. Based on this data a chi-square test was used to determine the significance of the data collected. IRB Approval (2016.71) was obtained prior to the start of data collection.
Results
In total there were thirty-three patients fit the inclusion criteria with fourteen females and nineteen males. There were twenty-three split thickness skin grafts, two full thickness skin grafts and eight flaps performed. Necessity of the procedure included traumatic injury, chronic non-healing wounds, burns, as well as fasciotomy sites. Conditions affecting wound healing (Chart 1) included a chronic opened wound bed (39%), cigarette smokers (33%) or some other medical condition affecting healing (51%) such as HIV, diabetes, peripheral vascular disease, cancer or alcoholism. A wound VAC device was placed on twenty-three (70%) of patients. There were no complications with twenty-two of the grafts or flaps, the complications that did arise included necrosis (9%), instability (6.1%), contracture (6.1%) and infection (3%). Additionally, there were five patients who had some other complication of their graft or flap. These complications included failure of a biologic allograft, infection of extremity prior to graft failure, recurrence of underlying cancer, iatrogenic graft displacement, and a non-healing ulcer in proximity to the graft. The average length of hospital stay overall was twenty-two days, patients receiving OMT had an average stay of twenty days. Overall there were four (one skin graft and three flaps) which failed. Twelve patients received at least one osteopathic treatment during their hospital stay. Once consulted, the OMT service saw each patient once every weekday for the duration of their hospital stay (range = 1 to 50 treatments). Of the patients receiving OMT none of the skin grafts or flaps failed X2 (2, N = 33) = 4.139, p = 0.126.
Discussion
While largely unknown, the rates of flap and graft failure varies greatly in the literature. It is important to illuminate forms of adjunctive care to prevent the failure of these procedures as there is an increased risk of infection, debilitating deformity, and prolonged limitation to functional status related to contractures and increased energy expenditures. 2
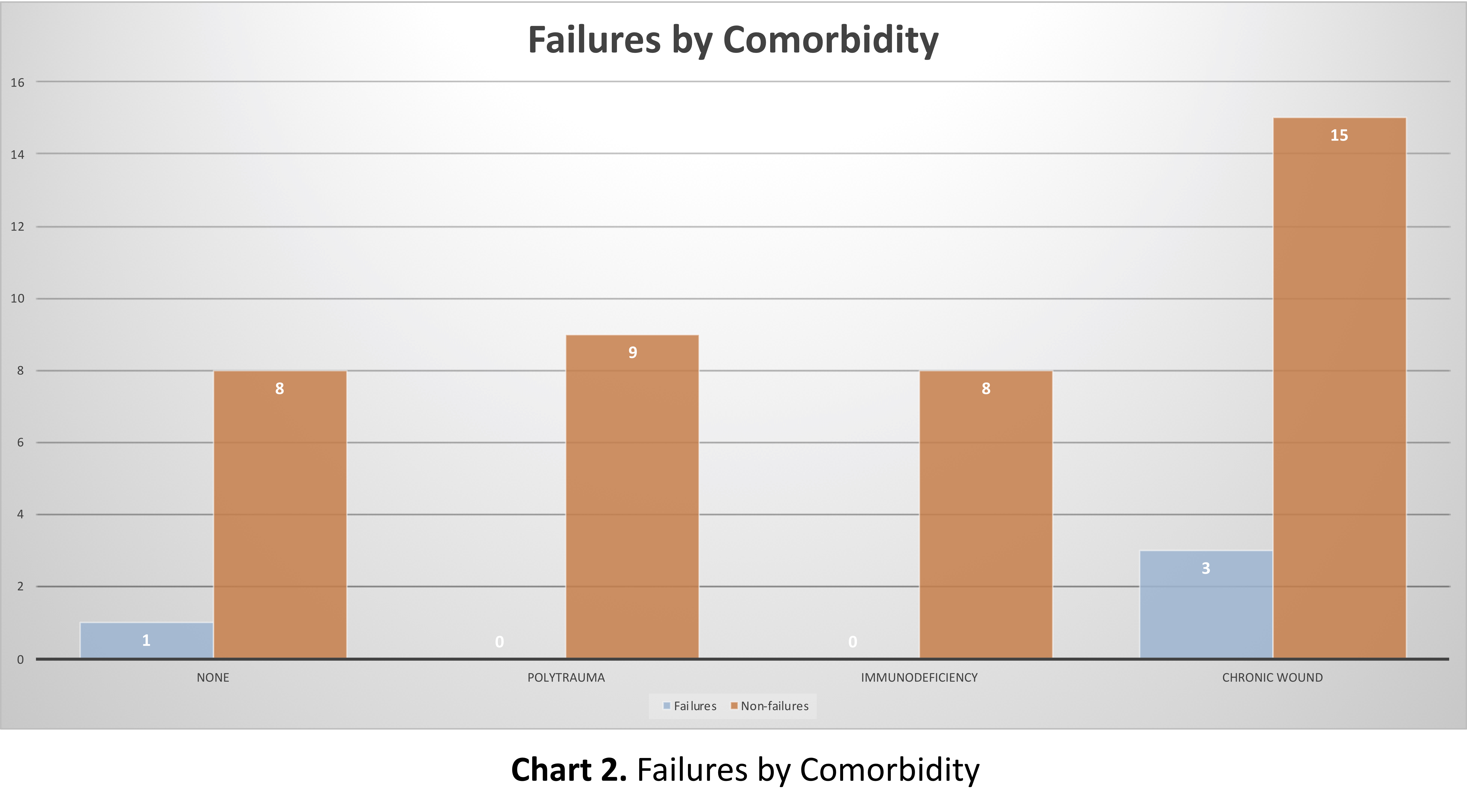
In the four cases of graft or flap failures, there were no patients who received OMT. Three of the failure patients had a chronic wound, adversely affecting healing. In a literature review, there are studies that show an improvement in healing times and tissue perfusion in patients for which OMT was used to augment the healing. 9 However, in the review of our data, only four of the fifteen patients with chronic wounds received OMT. This presents an opportunity for further research into the efficacy of OMT in patients with chronic non-healing wounds perhaps altogether avoiding a skin graft or flap surgery.
The average length of stay for a trauma patient in New York City is seven days. At this community based Bronx, NY hospital, the average length of stay is six and a half days. 10 In this study, the trauma patients who received OMT had an average hospital stay of twenty-five days. These patients sustained significant debilitating trauma necessitating multiple surgical interventions. The severity of injury is likely related to the increased length of hospital stay. The inclusion of OMT in the management of a patient with multiple traumatic injuries indicates an acknowledgement of the value that OMT provides to the trauma surgical service. In the same breath, the trauma patients exhibited no graft or flap failures. This further speaks to the efficacy of OMT in this setting. As some of the most critically ill patients in this study, these are the patients expected to have higher rates of complications. However, this has not been shown to be true within the scope of this study regarding those who received OMT. Of note, the patients who underwent a flap or graft who did not receive OMT had an average hospital stay of four days.
There are several limitations of this study which could be addressed with a formal prospective double blinded randomized controlled trials accounting for extraneous variables. The first limitation is the overall small sample size and the lack of even distribution between the intervention arm (OMT) and the control arm (non-OMT). This limitation could account for the lack of statistical significance. Additionally, while every attempt was made to case match patients based on medical conditions and complications that effect graft or flap healing this was not always possible. The uneven distribution of patients in each of the areas of associated complication (Chart 2) is a considerable limitation. Although there are OMT and non-OMT patients in each category, the study would benefit greatly with a larger study size.
There are three main phases of wound healing: inflammation, proliferation, and maturation. During the inflammatory phase, the main goals are hemostasis, sealing the surface of the wound, and removing any foreign material (i.e. necrotic tissue, bacteria, foreign bodies, etc). It is during this phase that there is increased permeability as well, mainly to increase the influx of various cells, chemokines, and other factors, but also causing capillary leakage of fluid to extracellular spaces. This phase usually lasts about four days after the initial injury, but overlaps with the second phase, which is proliferative. The proliferative phase is characterized by the formation of granulation tissue, through angiogenesis, fibroplasia, and epithelialization. This allows for the scaffolding of a more stable wound to mature around it. Lymphatic pathways are important during this phase as well to help with the movement of fluid to and from the wound as it progresses through each phase of healing. The proliferative phase usually lasts to two weeks post-injury. After the framework has been laid, the wound can then begin its maturation. During the maturation phase, the wound begins contracture, which is based on an increased scar tissue to normal tissue ratio. There is a slow, but continuous remodeling of the scar tissue that is built around the previously laid scaffolding, which is then replaced with new tissue of increasing strength. The maturation phase of wound healing is a long-term process that spans of the course of weeks, months, and years.
It is noted that during our retrospective chart review, the only flap and graft failures were within the non-OMT arm. There was a three-way cross tabulation analysis of the two groups, but due to the small population size and limited number of failures, the analysis was difficult and no statistically significant conclusions could be drawn. Although the efficacy of OMT on healing was not statistically significant, it can be anecdotally inferred that the manual intervention of OMT did not negatively impact the flaps and grafts, even in very recently postoperative patients. This allows for the open possibility of further research of the effects of OMT on newly postoperative patients, with little apparent risk to the surgical site.

Conclusion
As an understudied area, the utility of adjunctive therapies, such as OMT, in the success rates of skin grafts and flaps is severely limited. However, within the patient population and data set above, analysis demonstrated no skin graft or flap failures in patients who received OMT when compared to those who did not. Despite a lack of statistical significance, most likely due to a low study group number, the patient population necessitating skin grafts and flaps continues to grow and the rates of failure are varied with a wide range of causes. This potential allows for the validity and necessity of further retrospective, as well as prospective randomized control trials on a multicenter level to further evaluate the efficacy of OMT in this setting and control for variables affecting healing.
References
-
Ratner D. Skin Grafting: From Here to There. Dermatologic Clinics, 1998;16:75-90.
-
Oganesyan G, Jarell AD, Srivastava M, Jiang SI. Efficacy and Complication Rates of Full-Thickness Skin Graft Repair of Lower Extremity Wounds After Mohs Micrographic Surgery. Dermatol Surg, 2013;39:1334-1339
-
Reddy S, El-Haddawi F, Fancourt M, Farrant G, Gilkison W, Henderson N, et. al. The Incidence and Risk Factors for Lower Limb Skin Graft Failure. Dermatol Res and Prac, Epub 2014 Jul 15.
-
Weinzweig J. (2010). Plastic surgery secrets. Philadelphia, PA: Mosby/Elsevier
-
Townsend CM, Beauchamp DR, Evers MB, Mattox KL (2012). Sabiston Textbook of Surgery: The biological basis of modern surgical procedures (Nineteenth ed.). W B Saunders Company.
-
Neligan PC. (2013). Plastic Surgery (Third ed., Vol. 1). New York, NY: Elsevier.
-
Guyuron B, Chung KC. (2009). Plastic surgery: Indications and practice (First ed.). Edinburgh: Saunders.
-
Digiovanna EL, Schiowitz S, Dowling DJ. An Osteopathic Approach to Diagnosis and Treatment. Philadelphia, Lippincott Williams & Wilkins, 2005.
-
Leduc A, Lievens P, Dewald J. The influence of multidirectional vibrations on wound healing and on regeneration of blood-and lymph vessels. Lymphology, 1981;14:179-185.
-
New York State Department of Health. (n.d.). Retrieved February 26, 2017, from https://www.health.ny.gov/professionals/ems/state_trauma/
-
Leong M, Phillips L. (2012) Wound Healing. Sabiston Textbook of Surgery: The biological basis of modern surgical procedures (Nineteenth ed.). W B Saunders Company.