INTRODUCTION
A pneumothorax is a potentially lethal complication of patients on mechanical ventilation. Furthermore, timely identification of this complication and appropriate chest tube insertion can be life saving. However, to our knowledge, there are no established clinical guidelines for the management of patients on mechanical ventilation who have rapidly expanding bullous disease. We report a case of a patient with a rapidly expanding bulla on positive pressure ventilation.
CASE PRESENTATION
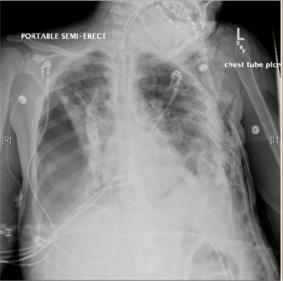
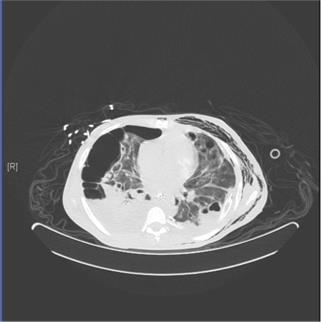
A 30 year old female with a history of intravenous drug abuse and hepatitis C was admitted with tricuspid valve MRSA endocarditis and associated septic pulmonary emboli. On admission she required intubation and mechanical ventilation for progressive respiratory failure. The initial chest xray demonstrated bilateral bullous disease, alveolar consolidations, and a small left pneumothorax for which a chest tube was inserted. Following 3 days of positive pressure ventilation the patient’s repeat chest xray demonstrated a significantly enlarging right lung bulla that occupied >50% of the hemithorax. Given the rapid rate of expansion of this bulla and the continued need for mechanical ventilation, a right-sided chest tube was preemptively inserted to avoid a potential deadly tension pneumothorax. The patient’s hospital course was subsequently complicated by a persistent right-sided bronchopleural fistula, for which she ultimately underwent placement of an endobronchial valve.
DISCUSSION
It is well known in the literature that positive pressure ventilation predisposes to pneumothorax formation in patients with underlying bullous lung disease. Additionally, it is clear that the development of a pneumothorax on mechanical ventilation requires urgent chest tube placement. However, it is less certain how patients with rapidly expanding bullae on positive pressure ventilation should be managed. We present a case in which a chest tube was preemptively inserted in such a patient. This intervention may have been life-saving, but did result in the complication of a persistent bronchopleural fistula. Further data is required to establish clear guidelines regarding this patient population.
Images




REFERENCES
-
Marini J, Wheeler A. Acute Complications Of Mechanical Ventilation. In: Critical Care Medicine: The Essentials, 4th ed. Philadelphia: Lippincott Williams & Wilkins, 2010: 149-159.
-
Barash P, Cullen B, Stoelting R, Cahalan M, Stock M. Lung Cysts and Bullae. In: Clinical Anesthesia, 7th ed. Philadelphia: Lippincott Williams & Wilkins, 2013: chapter 37.