ABSTRACT
Mycobacterium avium complex (MAC) infection is more commonly seen in patients with impaired immune system, associated with malignancy or foreign body in the lungs. This pathogen can cause mild hemoptysis, but massive hemoptysis is an atypical presentation of MAC infection that sometimes could require embolization of pulmonary arteries. This patient presented with recurrent MAC infection and massive hemoptysis with lack of some common risk factors such as impaired immunity, cancer, aspergillus co-infection or foreign body in the lungs. Massive hemoptysis in patients presenting with MAC infection is not common but could be life threatening if present.
INTRODUCTION
Diagnosis of Non-Tuberculosis Mycobacteria (NTM) infections represents a challenge to medicine professionals and to increase recognition of lung infections caused by NTM, physicians are required to be aware of this atypical group of organisms. NTM species include all Mycobacterium except M. tuberculosis, M. bovis, M. africanum, M. microti and M. leprae. 1 Some studies have shown that NTM causing pulmonary infection in non-HIV patients are mostly slow growing mycobacteria such as M. avium complex (MAC), M. kansasii and M. xenopi. 2 Recurrent MAC infection has been described in immunocompromised patients, with presence of foreign bodies, 3 ‘ 4 ‘ 5 ‘ 6 associated with lung cancer or chronic cavitation in the lung.
CASE PRESENTATION
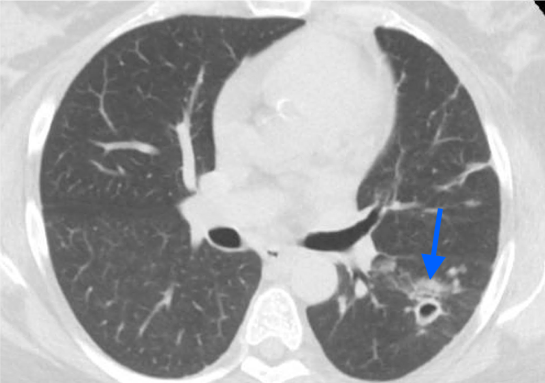
We present a case of a 55-year-old African American woman, who presented to the hospital at the end of 2019. The patient had a medical history of hypertension, diabetes mellitus, hyperlipidemia, moderate persistent asthma, left lung cavitation with positive Acid-Fast Bacillus test (AFB) and biopsy for MAC in 2016 (Treated with Ethambutol and Rifampin, completed treatment in December 2018) and stage I right lung adenocarcinoma with surgical resection in August 2017 (see blue arrow in image [fig. 1] , pre-resection CT). Also, previous pulmonary embolism, atrial fibrillation not ¬on chronic anticoagulation, recurrent strokes (2009, 2011, 2014) with no residual deficit. Her social history is relevant for smoking 15 packs per year, use of occasional recreational marijuana, crack and cocaine. She works as a security guard.
During late November 2019 she complained of 3 days of cough, sore throat and worsening fatigue with an episode of hemoptysis of approximately 200ml, reason why she visited the Emergency Department. Patient denied fever, weight loss, night sweats, chest pain, palpitations, chills, headaches or sick contacts. Admitted to critical care unit for massive hemoptysis. Among the workup done, she underwent a lung biopsy that yielded negative tissue results for either AFB’s or malignant cells. Initial blood work was relatively normal, except for hyperglycemia; however, an interval CXR revealed mild hazy air space opacification at the left mid to lower lung fields (see XR chest in image [fig. 2] ). Due to high risk for malignancy and history of mycobacteria infection a CTA chest was obtained, with positive results for mild interval enlargement of a previously seen left lower lobe spiculated nodular density within adjacent cavitary lesion with a new mild adjacent ill-defined patchy left pulmonary airspace disease (see Image [fig. 3] , green arrow). AFB stain of sputum reported 3/3 positive samples. Serum QuantiFERON TB resulted negative. Aspergillus fumigatus, Flavus and Niger antibodies were all negative. HIV test was non-reactive. CT scan guided needle biopsy showed: benign pulmonary tissue with focal fibrosis and one multinucleated giant cell, absence of granuloma and negative AFB stain. After the biopsy results and clinical suspicion, the patient was started on Rifabutin, Isoniazid, Pyrazinamide, Azithromycin and Ethambutol to cover MAC and MTB. Molecular testing of these samples showed Mycobacterium avium complex positive genotype and negative Mycobacterium tuberculosis. After PCR result, the treatment was narrowed to Rifabutin, Ethambutol and Azithromycin to be discharged home with outpatient follow up and complete treatment until cultures are negative at least for 12 months.
DISCUSSION
Pulmonary infections are a well known cause of massive hemoptysis, including Mycobacterium tuberculosis, mycetoma, lung abscess, parasitic infection, necrotizing pneumonia. 7 Although hemoptysis has been described in relation with MAC infection, massive hemoptysis is rarely seen, however has been described before. 8 ‘ 9 An epidemiological study conducted in Italy where they observed all adults admitted for massive hemoptysis for a period of 2 years found atypical mycobacteria to cause only mild hemoptysis; no moderate or massive hemoptysis were registered in this period of time. 10 Okuda et al 9 presented a study where they analyzed characteristics for patients presenting with massive hemoptysis and described importance of co-infection of Aspergillus, sometimes seen in these patients. Cavitation, nodular bronchiectasis in the lungs are a risk factor for Aspergillus and MAC infection in the lungs. 4 This patient’s cavitation predisposes her to NTM infection.
Lung cancer has a clear association with MAC infection. A case series in Japan showed that recurrence of MAC infection and lung adenocarcinoma needed to be differentiated 3 since some patients with recurrent MAC infection showed positive biopsy for malignancy afterwards. The Mayo Clinic in Rochester studied some factors as well associated with MAC infection in previously treated lung cancer patients; among these risk factors they found bronchiectasis, COPD, immunosuppression and a combination of these. 6 In this study there was a small group of people with no apparent risk factors besides history of lung cancer6 that presented with MAC infection. Hemoptysis is common in pulmonary MAC infection, but massive or large hemoptysis is an atypical presentation. A retrospective study in Japan analyzed bronchoscopies performed in lung cancer patients and found MAC/atypical mycobacteria in approximately 2% of cases, with a significant relationship established for older age, female sex and positive smoking history. 11 This relationship is independent on the timeframe of diagnosis as found in Lande et al, 12 where patients with pulmonary MAC infection were found positive for malignancy either before, at the moment or after the diagnosis. Since this relationship is very close, patients with pulmonary MAC infection and no other risk factors should be routinely screened for malignancy, especially in the settings of patients presenting with any sort of hemoptysis.
The present case of recurrent MAC infection related with fibro-cavitary lesion in a patient who had negative biopsy results for recurrent malignancy represents an uncommon case of MAC infection. This atypical presentation is due to the fact that she had no immunosuppression. More studies of risk factors for massive hemoptysis in MAC infection are needed, as well as lung cancer, active smoking and MAC association.
REFERENCES
-
Griffith DE. Overview of nontuberculous mycobacterial infections in HIV-negative patients. UpToDate: May 2020. Access June 6 2020.
-
Dailloux M, Abalain ML, Laurain C, Lebrun L, Loos-Ayav C, Lozniewski A et al. Respiratory infections associated with nontuberculous mycobacteria in non-HIV patient. Eur Resp J 2006;28:1211-15.
-
Al-Shaikhly T, Buckner FS, Altman MC, Ochs HD, Ayars AG. A 71-year-old man with recurrent pulmonary mycobacterial avium complex infections and lymphopenia. Allergy Asthma Proc 2020;41:66–69.
-
Goddard AG, Bathla G, Petts J, Ballas ZK. Recurrent Mycobacterium avium complex infection an unlikely case. Infect Dis Clin Pract 2017;25:e6–e8.
-
Kobashi Y, Abe M, Yoshioka D, Kato S, Oga T. Pulmonary Mycobacterium avium Complex Disease Requiring Differentiation from Recurrence of Lung Cancer during the Follow-Up Period for Lung Cancer. Journal of Tuberculosis Research 2019;7:220-227
-
Meier E, Pennington K, Gallo de Moraes A, Escalante P. Characteristics of Mycobacterium avium complex (MAC) pulmonary disease in previously treated lung cancer patients. Respiratory Medicine Case Reports 2017; 22:70e7371.
-
Kathuria H, Mollingsworth MH, Vilvendhan R, Reardon C. Management of life threating hemoptysis. Journal of Intensive Care 2020;8:23.
-
Adachi T, Ogawa K, Yamada N, Nakamura T, Nakagawa T, Tarumi O et al. Bronchial occlusion with Endobronchial Watanabe Spigots for massive hemoptysis in a patient with pulmonary Mycobacterium avium complex infection. Respiratory Investigation 2016;54:121-124
-
Okuda K, Masuda K, Kawashima M, Ando T, Koyama K, Ohshima N et al. Bronchial artery embolization to control hemoptysis in patients with Mycobacterium avium complex. Respiratory Investigation 2016;54:50-58.
-
Mondoni M, Carlucci P, Job S, Parazzini EM, Cipolla G, Pagani M et al. Observational, multicentre study on the epidemiology of haemoptysis. Eur Respir J 2018;51:1701813
-
Tamura A, Hebisawa A, Kusaka K, Hirose T, Suzuki J, Yamane A et al. Relationship Between Lung Cancer and Mycobacterium Avium Complex Isolated Using Bronchoscopy. The Open Respiratory Medicine Journal 2016; 10:20-28
-
Lande L, Peterson DD, Gogoi R, Daum G, Stamplet K, Kwait R et al. Association Between Pulmonary Mycobacterium Avium Complex Infection and Lung Cancer. J Thorac Oncol. 2012;7:1345–1351