Background
Traditionally, clinically significant pneumothorax and hemothorax secondary to trauma have been treated with a chest tube (28-36F) for evacuation of either air or blood respectively. In order to decrease the morbidity associated with tube thorocostomy many surgeons have now advocated the use of a small catheter (14F pigtail) that can be placed percutaneously utilizing a Modified Seldinger Technique. The pigtail catheter is typically placed under imaging guidance. Previously studies have been done and have shown no difference in the treatment outcome of small-bore pigtail catheters. Kulvatunyou N et al found that 14F pigtail catheters had no difference in outcomes for treating traumatic hemothorax [fig. 2] . A review of 49 articles in the journal of emergency medicine also found that small bore and large bore drains did not affect patient outcomes [fig. 3] . Balogh ZJ et al found that 38% percutaneous placed pigtail catheters resulted in some type of error1. There does not seem to be a consensus among physicians at this time regarding the usage of small-bore catheters for trauma patients. In this study we compared two groups of thoracic trauma patients who were either treated with a formal chest tube or a pigtail catheter without the use of imaging guidance.
Materials and Methods
This study is a IRB approved retrospective review of patients who required intervention for either traumatic pneumothorax or hemothorax. Our Trauma Registry was utilized to identify the study population and a chart review was performed to complete the data extraction. The outcome measures that were analyzed were: hospital length of stay (LOS), the length of time until removal of the chest tube or catheter (LOT) and the number of complications associated with each placement. From August 2011 to June 2013 a total of 89 patients underwent either a chest tube or pigtail catheter placement due to a traumatic injury. A total of 17 patients were excluded, 10 due to death, 3 were transferred to an outside facility, 3 had multiple tubes placed initially, and 1 underwent a drainage of a pleural effusion well into their hospital stay. Statistical analysis was done using a two-tailed Students T-Test with Microsoft Excel for Mac®.
Results
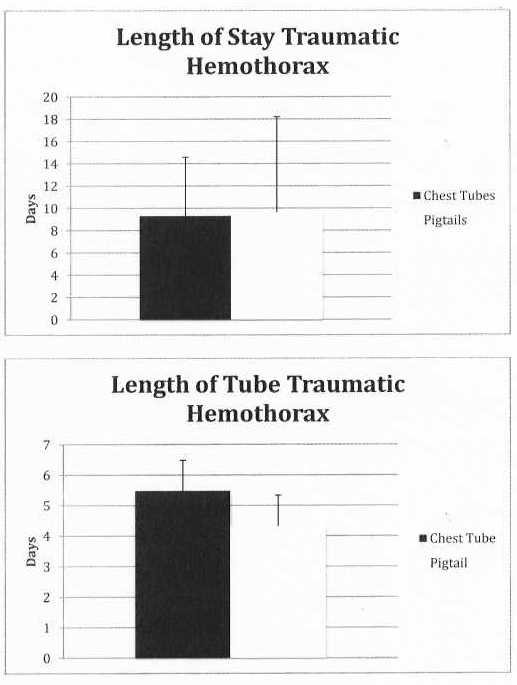
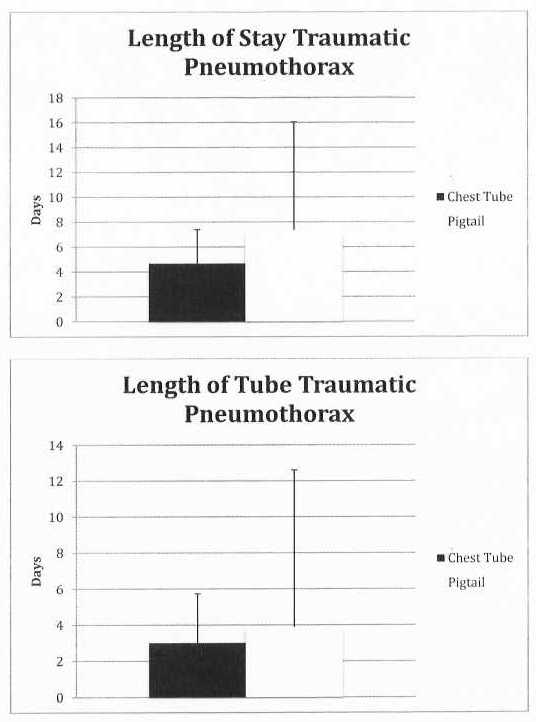
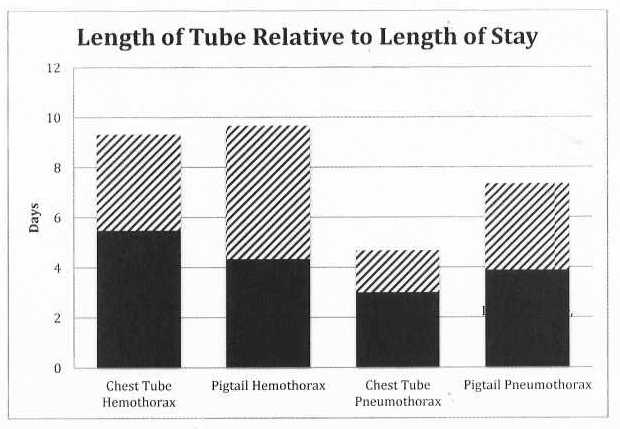
We found that the average Length of Stay (LOS) for all the patients was 8 days with a standard deviation of 7.31. The average Length of Tube (LOT) was 4.4 days with a standard deviation of 2.48. When comparing the LOS for pigtail verses chest tube in regards to patients with a hemothorax we found there to be no difference (p-value 0.89); there was also no difference when comparing the LOT (p-value 0.38). In regards to pneumothorax, again we noted there to be no difference in LOS or LOT (p-value 0.46 and 0.31 respectively). We also found that 29% of all Chest tubes placed had some type of complication, such as the need to place an additional tube, a tube placed into the lung parenchyma, or the need for a thoracotomy, compared to 7.32% of all Pigtails placed (See Table 2).
Discussion
Although this is a small retrospective chart review it seems that the use of a pigtail catheter placed percutaneously without image guidance may be a reasonable alternative to formal chest tube placement, as we found it to have equal effectiveness with decreased morbidity. Due to the nature of this study being a chart review and not a double-blinded randomized control trial the number of patients included in each group was very uneven. We believe that numbers of patients in each group were uneven due to each trauma surgeon’s personal preference when placing either a chest tube of pigtail. In the future we would like to further this study to increase the power by increasing the number of patients included in each group.
Table 1

Table 2