ABSTRACT
Amoebiasis is caused by protozoan Entamoeba histolytica. Amoebic liver abscess (ALA) is the most common extraintestinal manifestation of Entamoeba histolytica infestation and is associated with significant morbidity and mortality. There are various complications associated with ALA such as vena cava (IVC) thrombosis and pulmonary embolism. IVC thrombosis may result from the mechanical compression of the IVC or may be due to the thrombogenic nidus elicited from the resultant inflammatory response. We present a case of a 58-year-old male who presented with fever, right upper quadrant abdominal pain and hemoptysis. On work up, he had an amoebic liver abscess complicated by IVC thrombosis progressing to pulmonary embolism.
INTRODUCTION
Amoebiasis occurs in 10% of the world’s population and is most common in tropical and subtropical regions. 1 Low socioeconomic status and poor sanitary conditions and are the major factors responsible for the high incidence of liver abscesses in the Indian subcontinent. Inferior vena cava (IVC) thrombosis secondary to liver abscess is a very rare yet life threatening complication associated with amoebic liver abscess (ALA). There are very few reported cases of ALA complicated by IVC thrombosis and even fewer in which the IVC thrombus further leads to pulmonary thromboembolism. We present a case of ALA complicated by IVC thrombosis and pulmonary embolism.
CASE REPORT
A 58-year-old male, resident of Rohtak (India) presented with complaints of dull aching right upper abdominal pain and one month of fevers associated with chills and rigors. He complained of seven days of cough with red coloured sputum, shortness of breath and pedal edema. His past medical history is notable for treatment for ischemic cardiomyopathy.
On physical examination, the patient was febrile. Blood pressure was 110/70 mm Hg, pulse rate 110 and a respiratory rate of 40 per minute. He had pitting pedal edema in both lower limbs. There was mild pallor but no cyanosis, clubbing, lymphadenopathy. Jugular venous pressure was not raised. Abdomen was distended with ascites and tenderness in the right upper quadrant. On chest examination, air entry was decreased in the right and left infra scapular regions. Cardiovascular system was within normal limits.
Complete blood count was significant for hemoglobin of 11.5gm/dl, total leucocyte count of 17000 /mm3 with 88% neutrophils, platelet count of 2.5 x 109 /L and an ESR of 15 mm. Liver function tests and creatinine were normal. Chest X-ray showed consolidation in right middle zone and bilateral pleural effusion. Mantoux test was negative. Sputum culture was negative and no acid fast bacilli were seen on 3 repeated sputum examinations.
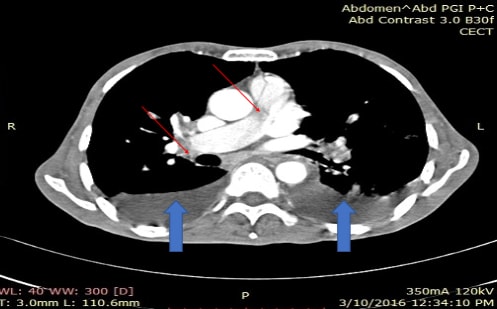
Ultrasound of the abdomen showed ascites and an enlarged liver with a hypo echoic area of 7.2 x 6.1 x 6.5 cm in the right lobe likely an abscess. CT of the abdomen showed free fluid in the peritoneal cavity and a hypodense peripherally enhancing lesion measuring 7.1 x 6.3 x 6.7 cm in the right lobe of liver suggestive of a liver abscess. A non-enhancing filling defect was noted in intrahepatic and supra hepatic portion of IVC suggestive of a thrombus with the abscess mildly compressing the vessel wall. [fig. 1] On chest CT, a non-enhancing filling defect was noted in right pulmonary and its lower branches suggestive of a thrombus along with bilateral effusions. [fig. 2] Echocardiography was notable for generalised hypokinesia of the left ventricle with an ejection fraction of 15%. An embolus was seen in right pulmonary artery.
Pleural and ascitic fluid analysis showed protein of 1.8 gm/dl and 2.0 gm/dl respectively, with no cells and ADA was negative. They were transudative in nature most likely due to cardiac dysfunction. Liver abscess was aspirated and it was reddish brown colored which resembled anchovy paste. There were no trophozoites seen on the microscopic evaluation of the abscess and no organisms were isolated on culture. The patient’s serum tested positive for amoebic antibody by enzyme linked immunosorbent assay (ELISA). Work up for underlying hypercoagulable states including factor V leiden, antithrombin III, homocysteine, protein C, and protein S. All values were all within normal limits and lower extremity duplex scan found no evidence of deep vein thrombosis.
The patient had a final diagnosis of amoebic liver abscess complicated by an IVC thrombus leading to pulmonary embolism and hemoptysis. He was treated with IV metronidazole for two weeks along with diloxanide furoate. He was discharged on warfarin with a regular follow up to maintain an INR between 2 and 3.
DISCUSSION
Amoebiasis is a protozoal infectious disease caused by an enteric parasite Entamoeba histolytica. It is the leading parasitic cause of death globally after malaria and schistosomiasis. 1 ALA is the most common extraintestinal manifestation of Entamoeba histolytica infection and can occur even in the absence of amebic colitis. 2 ALA results from the haemotgenous ascent of trophozoites of Entamoeba histolytica protozoa from the colonic mucosa to the liver through the portal venous system, which consequently leads to establishment of hepatic infection. The tropical and sub-tropical regions have the maximum prevalence of ALA. ALA should be clinically suspected in any patient with history of travel to an endemic areas and presenting with fever, right upper quadrant pain, and tender hepatomegaly. It is diagnosed radiologically by identifying a space occupying lesion in the liver most commonly by ultrasonography and a positive serum amoebic serology. Antibodies are seen in 90 to 100% of patients with ALA and become detectable seven to ten days after the onset of symptoms. For the diagnosis of amoebic liver abscess, amoebic serology has high sensitivity (>94%) and specificity (>95%). 3 Enzyme-linked immunosorbent assay and Indirect hemagglutination are the most commonly used serological method and have a high sensitivity. Negative pus cultures for entamoeba and non visualization of amoebic trophozoites in amoebic liver abscesses are a common finding seen in most of the cases. 4 Contrast enhanced computed tomography is an ideal investigation to particularly to detect smaller lesions and its associated complications with a high sensitivity of around 97%. 5
ALA can lead to life threatening infrequent complications such as rupture of the abscess into the pleural, pericardial and peritoneal cavity or bile duct. IVC thrombosis and pulmonary embolism are very rare complications and reported scarcely in the literature and are mostly described in autopsy studies. 6 IVC thrombosis complicated by pulmonary embolism can complicate the survival of the patient. 7 The exact pathophysiology of liver abscess complicated by IVC thrombosis and consequent pulmonary embolism is uncertain. The most common proposed mechanism is external compression of the IVC by the abscess along with a continuous spread of inflammation over the vessel wall. 8 , 9 This results in endothelitis and predisposition to stasis and thrombosis in the involved blood vessel. Vascular thrombosis can also be a result of the inflammatory processes associated with the amebic abscesses. Respiratory movements of the diaphragm and coughing can cause further damage to the endothelial lining of the IVC, thus enhancing the risk of thrombus formation. 10 Pulmonary embolism is usually secondary to IVC thrombus. In our case the likely mechanism of IVC thrombus was the mild external mechanical compression of IVC because of the abscess, resulting in a sluggish blood flow and initiating an inflammatory process in the wall of the amebic abscess leading to a prothrombic state in the vessel wall.
The management of complicated ALA is still controversial regarding surgery but most of the literature favors medical management. The management of ALA with IVC thrombosis depends on the extent of thrombus and the clinical condition of the patient. It includes antibiotics and drainage of the abscess. In a few cases, anticoagulation therapy is needed. If the only IVC is involved and thrombus has not progressed, drainage of abscess and antibiotics can relieve the mechanical compression of IVC and therefore there is no benefit of any anticoagulation. However, in this case, extension of thrombus lead to pulmonary embolism, therefore aggressive management in the form of anticoagulation was needed along with antibiotics. The duration of anticoagulation depends upon the resolution of abscess and associated thrombus. All the hypercoagulable causes for thrombosis must be ruled out. Radiological investigations should be repeated at timely intervals to see the resolution of the abscess and thrombus. Anticoagulation should be stopped when there is complete resolution of abscess and the thrombus.
This case of amebic liver abscess was unusual in that it was complicated by IVC thrombosis and pulmonary embolism. Management was antibiotics and anticoagulation. Timely intervention and therapy reduces morbidity and mortality.
Ethical Consideration
Patient consent form has been procured prior to the case report study after fully disclosing all points in local and English language.
Statement of Authorship
All authors have given approval to the final version submitted.
Author Disclosure
All the authors have declared no conflict of interest to the work carried out in this paper.
Funding Source
None
FIGURES
-
Fig. 1 – Thick (Blue) Arrow- Peripherally enhancing hypodense lesion measuring 7.1 x 6.3 x 6.7 cm in right lobe of liver suggestive of a liver abscess.
Thin (Red) Arrow- Non enhancing filling defect in intrahepatic portion of IVC suggestive of a thrombus with the abscess mildly compressing vessel wall.

-
Fig. 2 – Thin (Red) Arrow- Non enhancing filling defect was in right pulmonary and its lower branches suggestive of a thrombus
REFERENCES
-
Wells CD, Arguedas M. Amebic liver abscess. South Med J 2004;97:673-682.
-
Katzenstein D, Rickerson V, Braude A. New concepts of amebic liver abscess derived from hepatic imaging, serodiagnosis, and hepatic enzymes in 67 consecutive cases in San Diego. Medicine (Baltimore) 1982;61:237-246.
-
Zaman S, Khoo J, Ng SW, Ahmed R, Khan MA, Hussain R, et al. Direct amplification of Entamoeba histolytica DNA from amoebic liver abscess pus using polymerase chain reaction. Parasitology research. 2000;86:724-28
-
Halvorsen RA, Korobkin M, Foster WL, Silverman PM, Thompson WM. The variable CT appearance of hepatic abscesses. AJR Am J Roentgenol 1984;142:941-46.
-
Krishnan K, Badarinath S, Bhusnurmath SR. Vascular complications of hepatic amoebiasis-a retrospective study. Indian J Pathol Microbiol 1986;29:293-96.
-
Thati V, Nagral S. Inferior vena cava thrombus with pulmonary embolism complicating amebic liver abscess. Indian J Gastroenterol 2014;33:299
-
Sodhi KS, Ojili V, Sakhuja V, Khandelwal N. Hepatic and inferior vena caval thrombosis: Vascular complication of amebic liver abscess. J Emerg Med 2008;34:155-7.
-
England RA, Wells IP, Gutteridge CM. Benign external compression of the inferior vena cava associated with thrombus formation. BJR 2005;78:553-7.
-
Okuda K. Obliterative hepatocavopathy-inferior vena cava thrombosis at its hepatic portion. Hepatobiliary Pancreat Dis Int 2002;1:499-509.